Human Authority Over AI
The clinician stays in charge. Always.
HCP-as-Pilot™ — the umbrella clinical authority model. Physician-as-Pilot™ is the senior-clinician sub-pattern.
Implementing AI in a clinical environment? We'd love to hear your challenge.
Phase II · Physician-as-Pilot (sub-pattern of HCP-as-Pilot)
Tightly-bounded Agentic Orchestration enables a Safe Continuum of Care.
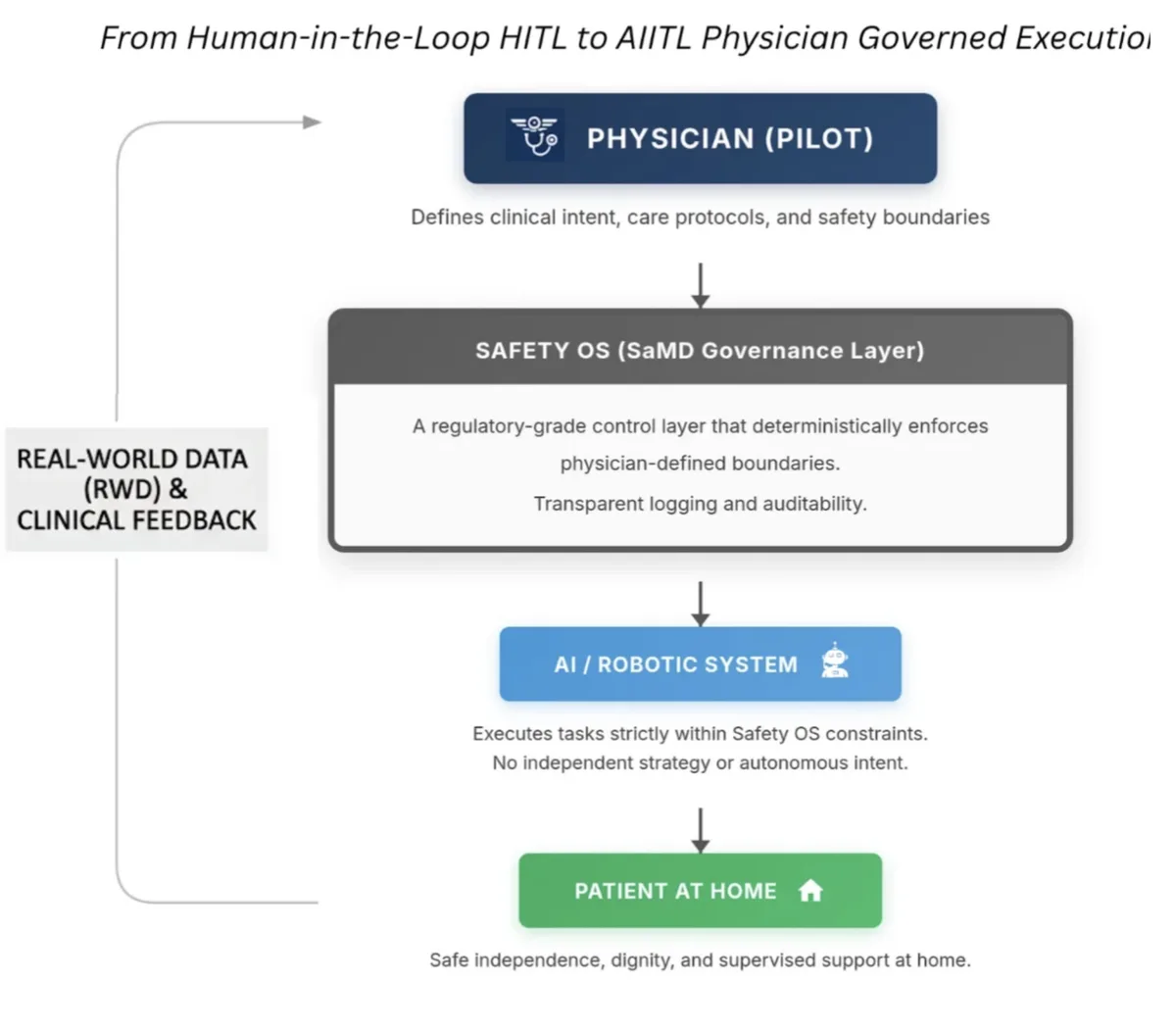
One governance envelope. From the clinic, through discharge, into the home. The physician is in command of every AI action — drafts, orders, follow-ups, coordination — and Phase I (Care Delivery Teams: nurses, caregivers, family) operates under the same Safety OS™ RGI rules. Every action consent-gated, audit-logged, and EU AI Act Article 14 aligned.

Safety OS™ does not replace AI systems, EHRs, or workflows. It governs the execution path between AI output and patient-impacting action.
Phase I (Care Delivery Teams) live today. Phase II (HCP-as-Pilot) ready for clinical environments. See the full architecture →
Modern healthcare AI fails not because models are weak, but because authority is unclear.
Physician-as-Pilot is the governance architecture that ensures AI systems never exceed human clinical authority - even as they scale toward regulated use.
Most AI governance relies on guidelines, training, and post-deployment monitoring. These approaches fail in regulated clinical contexts because they assume compliance rather than enforce it. Physician-as-Pilot enforces authority structurally - before execution, not after harm.
Citable Research
The governance architecture behind the Physician-as-Pilot model is described in the SSRN preprint:
Physician-as-Pilot Framework 2.1
A Phased Safety OS™ Governance Infrastructure for AI-Mediated Home Care and AIaMD
- • Selected as Best Overall Capstone - Harvard Medical School AI in Healthcare, 2026
- • Published as a preprint on SSRN
Read the Paper →
Physician-as-Pilot operating model. AI execution is governed by clinician authority through Safety OS constraints. Does not imply autonomous clinical decision-making.
What AI May Not Do Under This Model
- No diagnosis
- No treatment decisions
- No autonomous clinical intent
Clinical authority is never delegated to AI.
"Authority is a system variable - not a policy statement."
This principle forms the basis of the Physician-as-Pilot governance framework (SSRN preprint).
Liability Protection Through Reconstructible Authority
The Safety OS™ Flight Recorder provides a reconstructible record of authority state at the moment of any incident — including consent gate status, boundary class, escalation triggers, and human authority retention.
This enables post-incident reconstruction of exactly who held authority, what constraints were active, and whether escalation pathways were followed — providing clinical shielding through infrastructure, not policy.
Frequently Asked Questions
How is Physician-as-Pilot different from "human-in-the-loop"?
Human-in-the-loop (HITL) assumes AI acts first and a human reviews after. Physician-as-Pilot inverts this: the physician holds binding authority before AI can act in clinical domains. AI operates within pre-defined boundaries — it never exceeds what it has been explicitly authorised to do. This isn't oversight. It's governance by design.
What clinical settings does this apply to?
Phase 1 is deployed in home care settings supporting elderly patients. The framework is designed to scale across any clinical environment where AI assists in care — from home health to outpatient clinics to hospital wards. The governance principles (authority partitioning, bounded autonomy, deterministic escalation) are universal.
Does this slow down AI-assisted care?
No. Safety OS operates at runtime — governance checks happen in milliseconds. For non-clinical tasks (reminders, companionship, information), AI acts freely within its boundaries. Escalation only triggers when AI encounters something outside its authorised scope. The result is faster safe care, not slower care.
How does this align with the EU AI Act?
The EU AI Act (enforceable August 2, 2026) requires high-risk AI systems to maintain human oversight, demonstrate accountability, and provide audit trails. Physician-as-Pilot is designed to satisfy these requirements structurally — governance is enforced at runtime, not applied retrospectively. Safety OS generates the compliance evidence regulators will require.
What evidence supports this approach?
The framework was selected as Best Overall Capstone at Harvard Medical School's AI in Healthcare programme (February 2026). The full governance architecture is published as an SSRN research preprint. Phase 1 deployment generates real-world governance evidence in live care settings. See the Evidence & Milestones page for details.